

Abstract
Background: Idelalisib (IDEL) is a phosphatidylinositol-3 kinase (PI3K) inhibitor approved as a single agent for treatment of relapsed follicular lymphoma (FL) and in combination with rituximab for treatment of relapsed chronic lymphocytic lymphoma (CLL). The clinical trials supporting IDEL approval excluded patients with many comorbidities. We sought to investigate whether higher comorbidity burden among real world (RW) patients receiving IDEL might lead to differences in treatment duration, overall survival, or infection rates compared to clinical trial (CT) subjects.
Methods: CT data from the sponsor and RW data from Medicare were obtained for patients aged ≥65 years receiving: 1) IDEL monotherapy for FL or 2) IDEL with rituximab (IDEL+R) for CLL. A pretreatment modified Charlson Score (mCS; Quan H, 2011) was calculated using medical records for CT subjects and diagnostic reimbursement codes for RW beneficiaries. Treatment duration for IDEL was calculated from treatment start until the last patient contact for CT subjects and until the final day supply for RW beneficiaries. Overall survival was obtained from intention to treat data for CT subjects and through linkage to Social Security for RW beneficiaries. Serious infections were coded as Grade ≥3, as a serious adverse event, or required intravenous antibiotics for CT subjects. For RW beneficiaries, serious infections were obtained through manual abstraction of hospital discharge diagnoses or coded with intravenous antibiotics in emergent care. Fatal infections were defined as serious infections within 30 days prior to death. Results are reported descriptively and using Cox Proportional Hazards Models, adjusted by age, gender, mCS, and US location. Statistical modeling was intended to describe the generalizability of CT results to unselected RW population.
Results: A total of 26 CT subjects aged ≥65 years receiving IDEL monotherapy for FL from Study 101-09 were compared to 305 RW beneficiaries aged ≥65 years receiving IDEL for FL. A total of 89 CT subjects aged ≥65 years receiving IDEL+R for CLL in Study 312-116/117 were compared to 294 RW beneficiaries aged ≥65 years receiving IDEL+R for CLL. Key clinical comparisons are presented in the table below.
Age and mCS
RW beneficiaries receiving IDEL for FL had more patients ≥75 years (54% vs 35%) and with a mCS >3 (52% vs 12%) than CT subjects.
RW beneficiaries receiving IDEL+R for CLL had more patients ≥75 years old (52% vs 36%) and with a mCS >3 (52% vs 24%) than CT subjects.
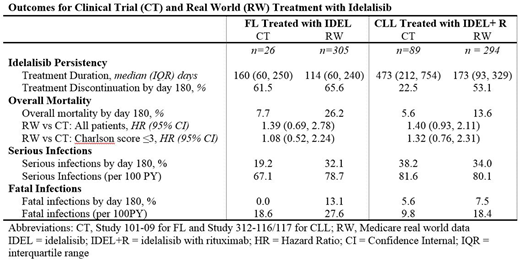
Idelalisib Persistency
CT subjects had a longer median idelalisib treatment duration and a lower treatment discontinuation rate by day 180 compared to RW beneficiaries. Differences were more pronounced for CLL.
A nonlinear, convex relationship was observed between mCS and treatment discontinuation among RW beneficiaries, indicating a higher mCS predicts more (than linearly expected) reduction in treatment duration. Few CT subjects had a mCS >3.
Overall Survival
Mortality was numerically worse for RW beneficiaries with FL (HR 1.39 95%CI: 0.69-2.78) or CLL (HR 1.40 95%CI: 0.93, 2.11) compared to CT subjects.
Among RW beneficiaries, each 1-point increase in mCS predicted a 10% (95%CI: 1.06, 1.14) increase in overall mortality for FL and CLL. Among CT subjects with CLL, mortality was worse for subjects with mCS >3 than for subjects with mCS ≤3 (HR 2.25, 95%CI: 1.13-4.49). Analysis of mCS among FL subjects had insufficient sample size.
Serious Infections
Serious infections occurred more frequently by day 180 in RW beneficiaries than CT subjects for FL (32.1% vs 19.2%) but not for CLL (34.0% vs 38.2%).
RW beneficiaries had higher rates of fatal infections for both FL (27.6/100PY vs 18.6/100PY) and CLL (18.4/100PY vs 9.8/100PY) compared to CT subjects.
Conclusions: The RW beneficiaries were older and had higher comorbidity burden compared to subjects ≥65 years included in CTs. RW beneficiaries had a shorter treatment duration, higher mortality rates, and higher fatal infection rates than CT subjects. Higher comorbidity, as measured through a pretreatment mCS, was associated with worse study outcomes. CT inclusion and exclusion criteria should allow enrollment of patients who are representative of the intended treatment population to maximize generalizability of CT results.
Acknowledgment: Clinical trial data provided by Gilead Sciences, Inc.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal